Glaucoma Surgery and MIGS
Glaucoma Laser
A selective laser trabeculoplasty (SLT) and argon laser trabeculoplasty (ALT) are both very similar laser procedures to reduce the eye’s pressure. This is done in the office by placing a special contact lens on the eye. The laser is then focused through this lens to the angle of eye (trabecular meshwork). The laser helps improve aqueous outflow which in turn helps reduce the eye’s pressure.
Goniotomy
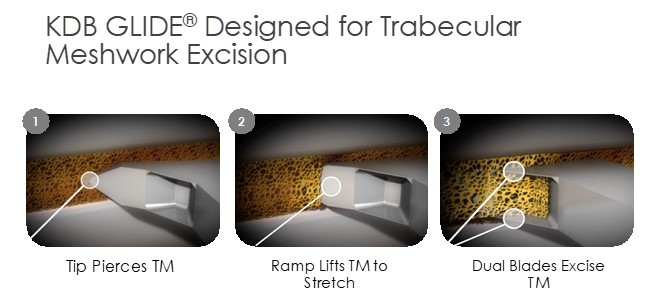
A Goniotomy is a Minimally Invasive Glaucoma Surgery (MIGS) which can lower intraocular pressure by improving the outflow dynamics of the eye. It was originally used to treat Glaucoma in children, but has been adapted to treat mild to severe Glaucoma in adults.
A Goniotomy opens the eye’s natural fluid drainage pathway by removing part of the trabecular meshwork. By opening the eye’s natural fluid drainage pathway, the intraocular eye pressure should decrease. There is no need for a stenting device with this procedure. A Goniotomy can be performed with or without Cataract Surgery. The post-operative care and follow-up is similar to Cataract Surgery.
The most common instrument to perform a Goniotomy is a KDB Glide. Below is a diagram demonstrating the removal of the trabecular meshwork.
Treating Your Glaucoma with an iStent
The iStent® is yet another way to treat mild to moderated glaucoma. The FDA requires this procedure to be performed in conjunction with cataract surgery. If you have already had cataract surgery you are not a candidate for this procedure.
If you have glaucoma, over time your eye’s natural drainage system becomes clogged. iStent® creates a permanent opening through the blockage to improve the eye’s natural fluid outflow. By improving the outflow of fluid in your eye, iStent® is designed to lower and control the pressure within your eye.
The iStent® Trabecular Micro-Bypass Stent is 20,000 times smaller than the intraocular lens (IOL) your doctor will use to replace your cataracts. By increasing your eye’s ability to drain fluid, this technology is designed to improve the aqueous outflow to safely lower your eye pressure.
If you are a candidate for the iStent® then your surgeon can implant it during your cataract surgery procedure. Once implanted, the iStent® will begin working to safely and effectively manage your eye pressure.
See How iStent Works
What is a Trabeculectomy?
A trabeculectomy is a glaucoma surgery that creates a small hole in the anterior chamber of the eye to allow drainage of the aqueous fluid toward the outside. Trabeculectomy surgery starts with making an incision through the conjunctiva. Underneath the scleral flap, a surgeon cuts a small hole into the anterior chamber, which allows the drainage of aqueous fluid through the scleral flap and into the sub-conjunctival space. An iridectomy (hole in the iris) is performed at this point to allow the scleral opening to stay open without being blocked by the iris tissue. The scleral flap is then tied down with stitches, that are loose enough to allow continuous drainage of the aqueous fluid. Finally, the overlying conjunctival tissue is closed with stitches to allow formation of a bleb or an elevation of conjunctival tissue formed by the aqueous fluid, which is being filtered out of the scleral flap (trapdoor) underneath. The filtering bleb is usually located in the superior aspect of the eye and covered by the upper lid. It is not readily noticeable by a casual observer. The aqueous fluid from the filtering bleb is then slowly absorbed by the conjunctival and episcleral (on the surface of the sclera) blood vessels and drain into the orbital venous system.
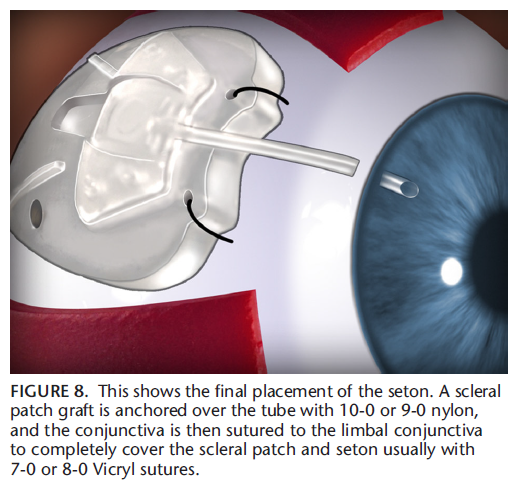
What is a Seton Implant?
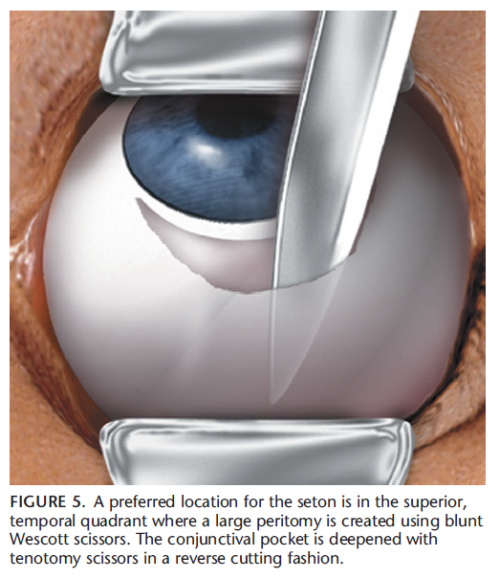
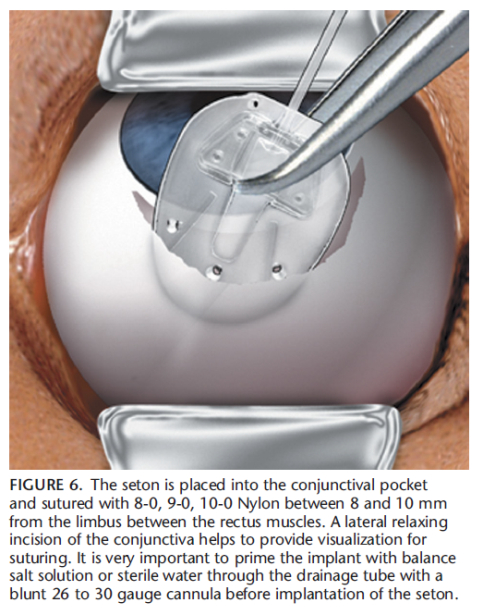
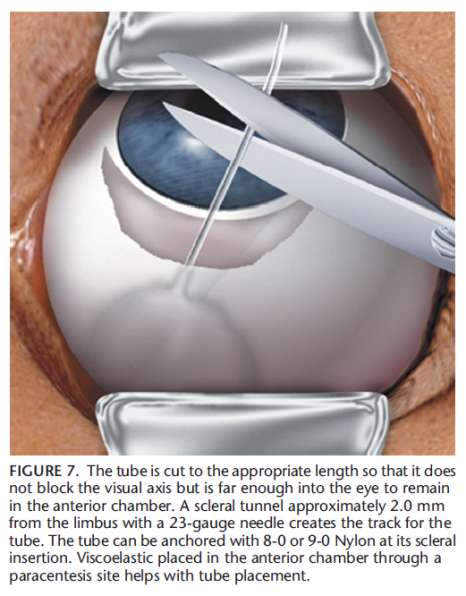
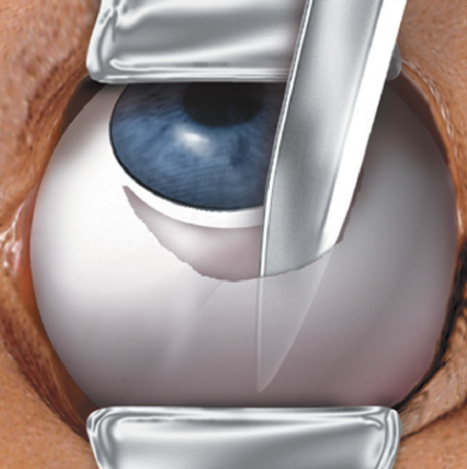
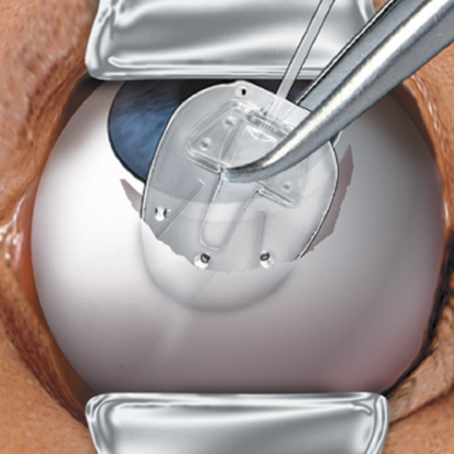
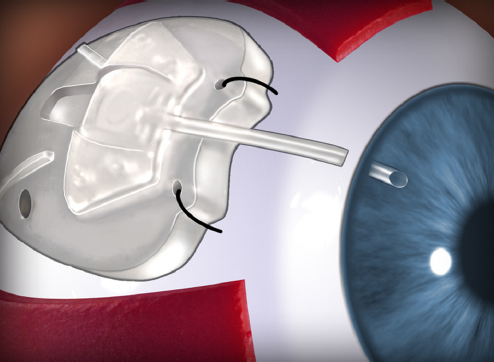
The seton implant is similar to a trabeculectomy, in that the goal is to decrease the eye’s pressure, by creating a pathway for the fluid inside the eye (aqueous fluid) to drain to the outside. A tube is inserted into the anterior chamber so the aqueous fluid can drain into the seton implant and out of the anterior chamber of the eye. The implant is sutured into a conjunctival pocket and the aqueous is absorbed naturally.
The diagram below shows the step-by-step insertion of a Ahmed Valve ® which is one of the most common seton implants.
The pictures below show the step-by-step insertion of a Ahmed Valve ® which is one of the most common seton implants.
Trab # 1
Trab # 2

Trab # 3
Trab # 4
Laser Eye Surgery of Erie
Additional Services
PTK and Amniotic Tissue Graft
Home Phototherapeutic Keratectomy (PTK) Phototherapeutic Keratectomy (PTK) and Amniotic Membranes with bandage contacts play an important role in treating…
read more
Corneal Transplants
Corneal transplants are required for a number of corneal diseases and a variety of other reasons. Before and after transplant,…
read more
Dry Eye
Dry eye occurs when people don’t produce enough tears or the right quality of tears to keep their eyes healthy…
read more
Diabetic Services
Diabetic retinopathy is a disease that affects diabetic people and eventually leads to blurry, distorted vision and blindness. When people…
read more
Macular Degeneration
Age-related macular degeneration (AMD) is a deterioration or breakdown of the eye’s macula. The macula is a small area in…
read more
Glaucoma Surgery and MIGS
iStent works like the stents used to prevent heart attacks and strokes. When blood vessels get clogged, a stent creates…
read more
Retinal Surgery
The retina is a thin sheet of nerve tissue in the back of the eye where light rays are focused…
read more
Keratoconus & Corneal Cross Linking
Keratoconus, often referred to as ‘KCN’, is a non-inflammatory eye condition in which the typically round dome-shaped cornea progressively thins…
read more
Glaucoma
Although glaucoma is the leading cause of blindness in Americans, early detection can prevent you from losing your eyesight. In…